Probe Guide
In an effort to increase the use of REM in clinical practice and to aid clinicians with obtaining proper probe tube insertion depth, Audioscan has developed Probe Guide. This clinically feasible, software-driven, acoustic-based tool was developed using a patent-pending machine-learning algorithm to guide probe tube placement in real time.
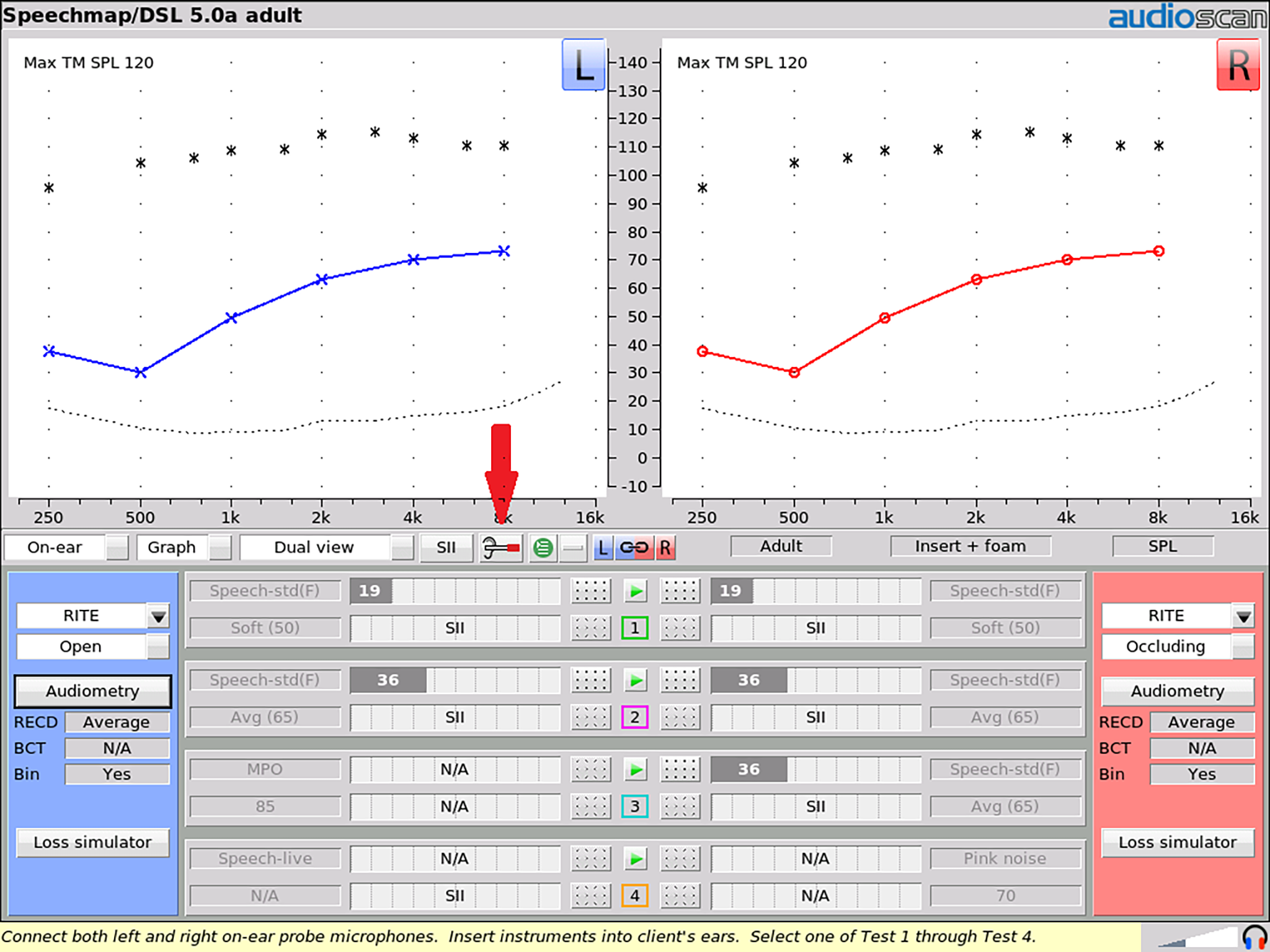
Figure 1. Probe Guide is accessed using the highlighted icon button on any on-ear test screen.
While a broadband noise signal is presented from the REM loudspeakers, the spectrum of sound within the ear canal is repeatedly sampled, analyzed, and input into a model of probe tube depth developed from a previously measured set of in-ear recordings. These recordings were gathered with normal adult ear canals as the probe tube was advanced to the correct location relative to the tympanic membrane.14 The machine-learning algorithm was “trained” to estimate probe tube depth from a sequence of input spectra, resulting in a software system that detects correct probe placement in real time.
A typical next step in machine-learning tool development is to test the trained system on a new dataset to evaluate whether the trained system works on new patients. Therefore, the purpose of the following collaborative study was to validate the performance of Probe Guide on a new set of ears. Our goal was to determine the performance of this new tool by comparing measured probe tube insertion depths between Probe Guide and a clinician-appraised depth, the adequacy of REMs made with Probe Guide, and the presence of any procedural issues (eg, eardrum contact) obtained with Probe Guide (PG) versus an experienced audiologist using a traditional visually assisted (VA) method of probe tube placement.
How to Use Probe Guide
Probe Guide can be accessed on any on-ear test screen on Audioscan Verifit2 (software version 4.18 and later) and Axiom (software version 1.24) by clicking the provided icon button (Figure 1). The guidance in probe tube placement is shown in Steps 1-3 below (Figures 2-4).
STEP 1: Setup
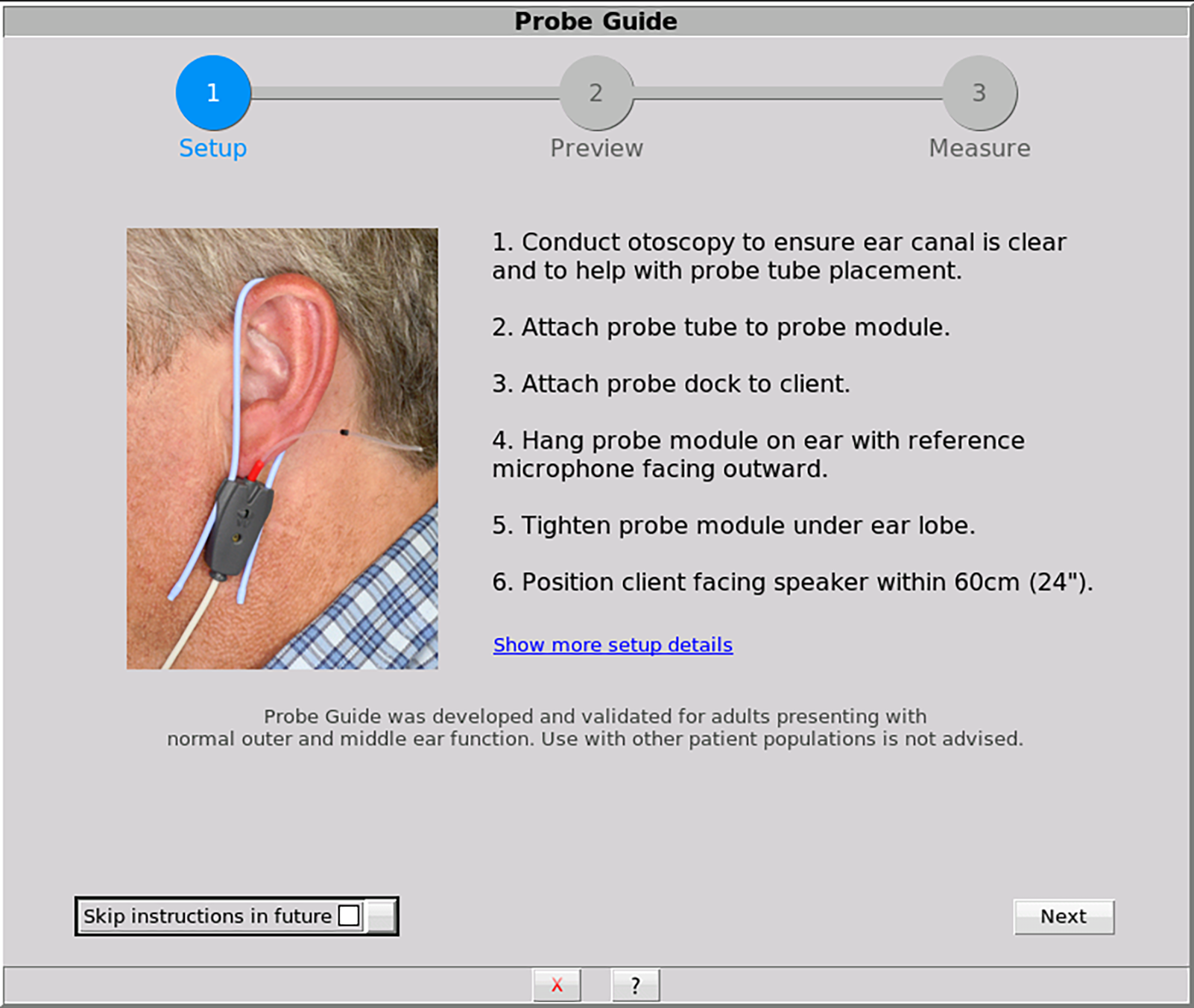
Figure 2. This optional screen describes methods for preparing the client and the equipment for probe tube placement
STEP 2: Preview
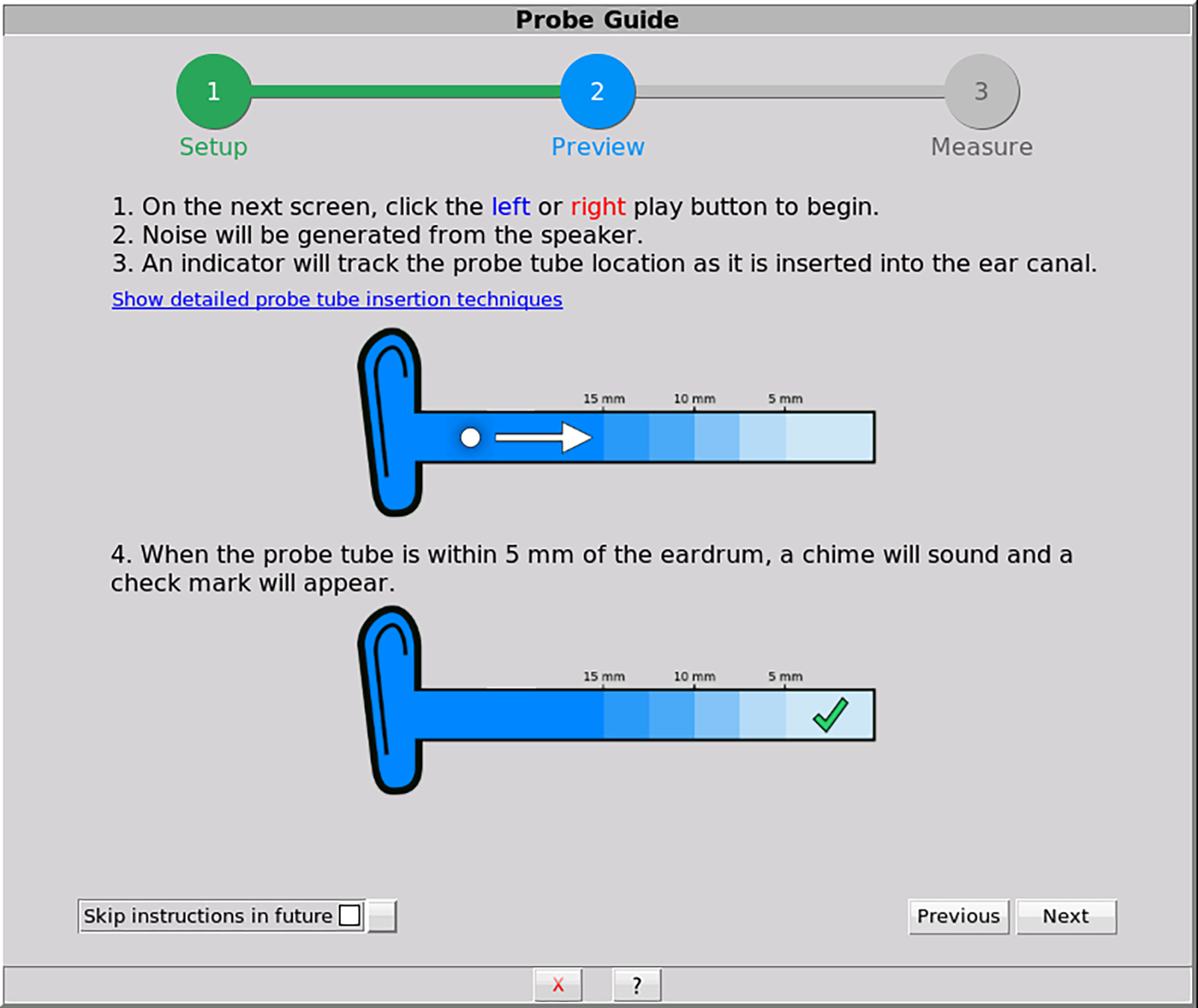
Figure 3. This optional screen describes procedural details on using Probe Guide to support proper use and counseling.
STEP 3: Measure
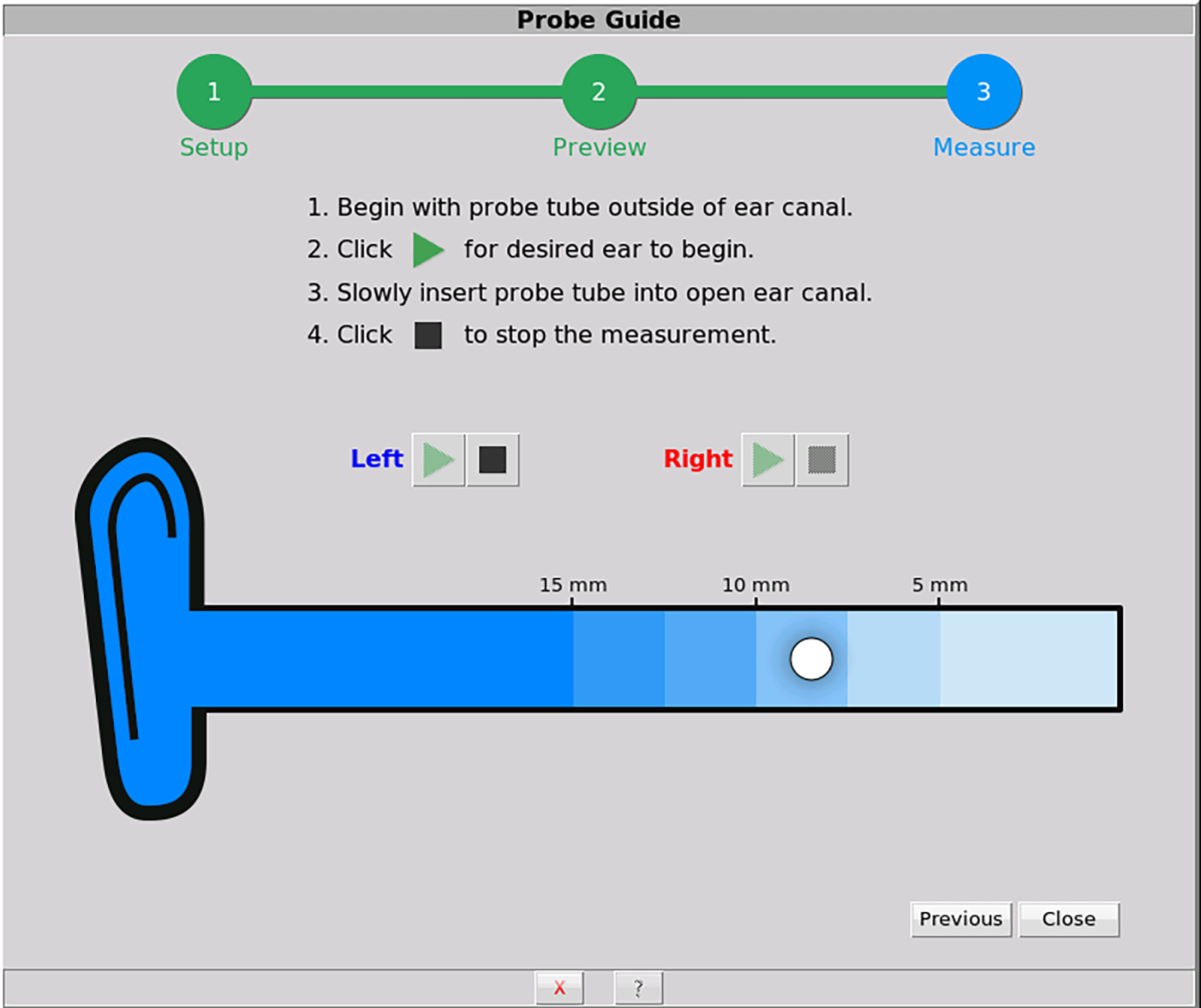
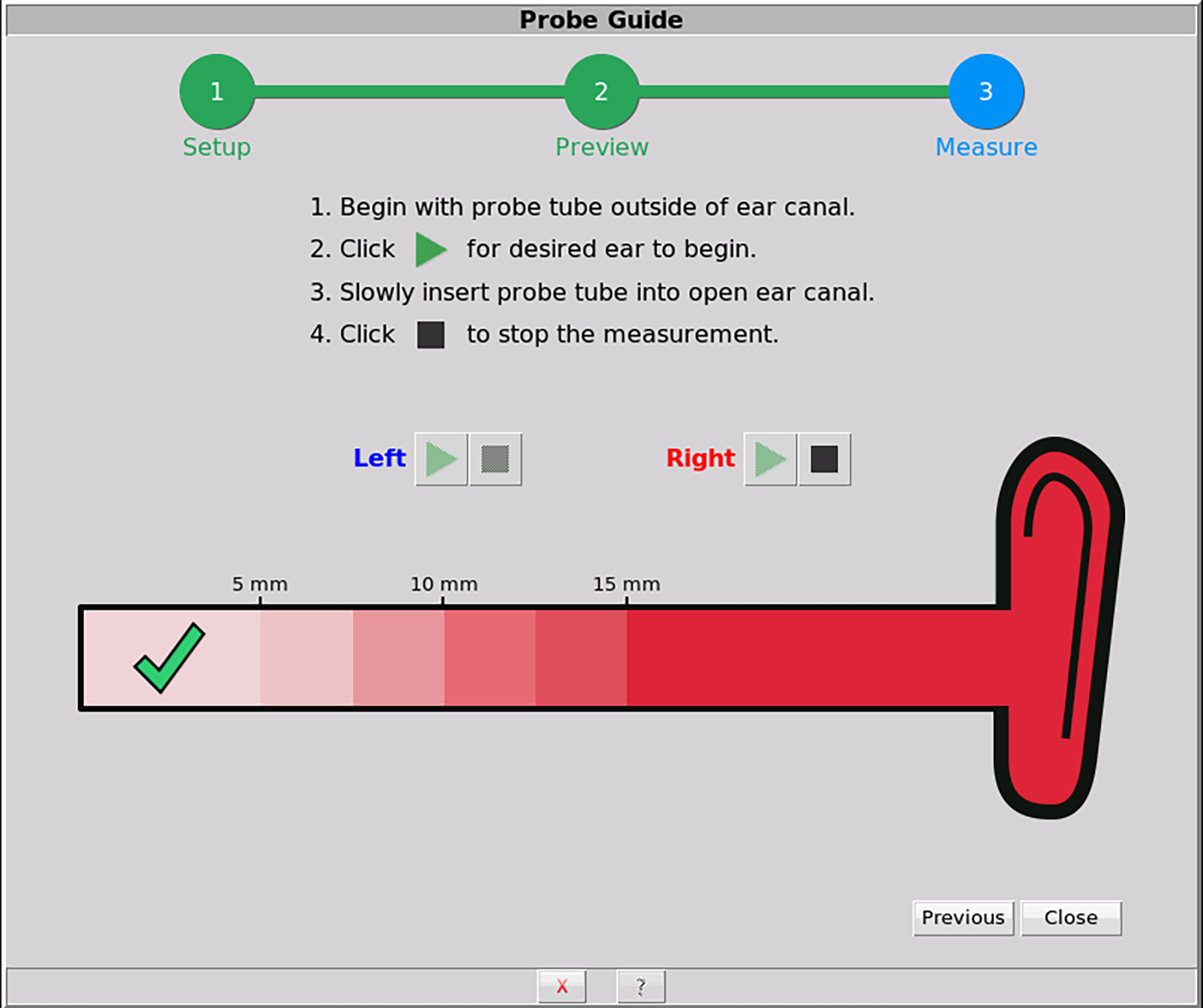
Figures 4a-b. This screen is used when performing the guided probe tube placement. A white ball tracker indicates real-time location of the probe tube. A green check mark and a chime is generated when the probe tube is within 5 mm of the eardrum.
Probe Guide Validation Study
The current study investigated the performance of the software-assisted Probe Guide method as implemented on Verifit2 relative to an expert clinician’s probe tube placement using the traditional visually assisted positioning technique. The expert clinician had more than 20 years of experience placing probe tubes for both clinical and research purposes.
Evaluation measures for each placement method included absolute probe tube insertion depth, test-retest reliability of probe tube insertion depth, real-ear unaided responses (REUR), and the occurrence of any procedural concerns (eg, patient discomfort, visual acceptability of placement, reported eardrum contact). A total of 20 participants (10 males and 10 females, ages 25-81) completed the protocol. All subjects had normal middle ear and external ear canal status as determined by otoscopy and impedance measurements.
Probe tube placement was completed on 40 adult ears, twice using the visually assisted method, and twice using Probe Guide. The starting order was counterbalanced across ears and placement methods. A within-subjects design was used to measure these system performance variables at the individual level. The probe tube marker, typically used to aid with probe tube placement, was moved to the base of the probe tube so as not to influence insertion depth decision-making.
For the visually assisted method, the probe tube was placed considering anatomical markers that correspond to a distance of approximately 5 mm from the tympanic membrane. The clinician used otoscopy to monitor the probe tube location. For the software-assisted method, the probe tube was inserted until Probe Guide indicated the proper insertion depth had been achieved.
Following probe tube placement with either method, the REUR was measured using a 65 dB SPL pink noise following the standard ANSI S3.46-2013 REM procedure. Next, the probe tube was marked with a fine felt tip pen at the intertragal notch. The probe tube was then removed from the ear canal and the distance from the medial end of the probe tube to the marked line was measured to calculate the insertion depth in millimeters. The mark was removed and the procedure was repeated again to evaluate test-retest reliability. The procedure was completed twice in each ear canal resulting in 4 measurements for each participant (Figure 5).
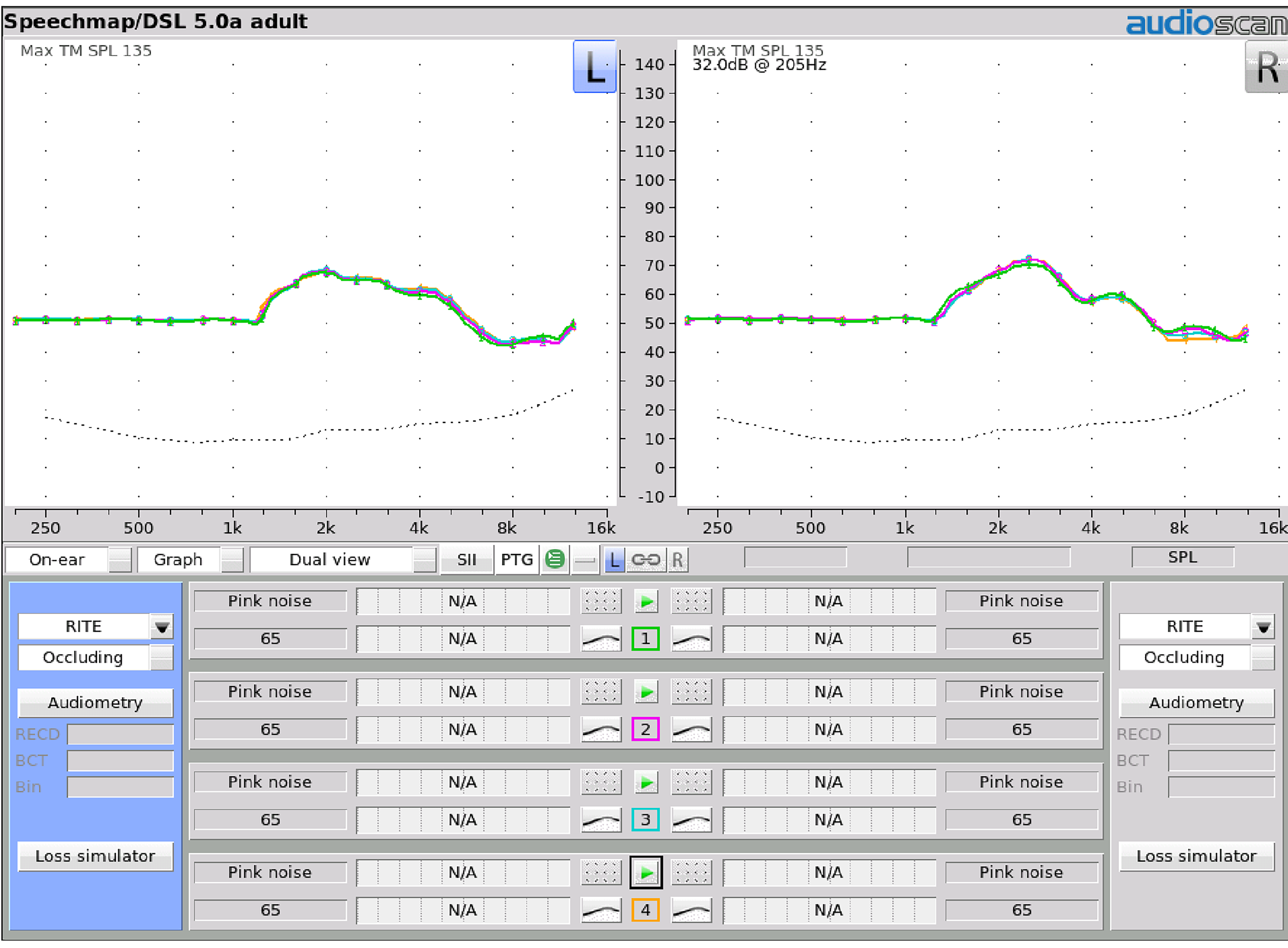
Figure 5. Real-ear unaided response (REUR) measures for one participant. Four REUR measures were completed for each ear. (Test 1 – Visually assisted (VA); Test 2 – VA (second run for test-retest); Test 3 – Probe Guide (PG), and, Test 4 – PG for test-retest).
The Speechmap session files from the Verifit2 were saved and exported in .xml format and imported into a spreadsheet for further analysis. The acoustic differences between the visually assisted and Probe Guide methods were calculated at all 1/12th octave frequencies measured by the Verifit2.
Results
Real-ear unaided response (REUR) measurements.
Group data were analyzed for the 20 participants. All statistics were completed using SPSS v24. A repeated measure analysis of variance (ANOVA) was completed to evaluate differences between probe tube placement methods for: 1) Probe tube insertion depth, and 2) REURs. In addition, within each probe tube placement method, test-retest reliability was evaluated. If significant differences were revealed, post-hoc paired comparisons were completed with Bonferroni corrections.
The ANOVA was completed comparing the results from the two methods, with left and right ears and repetitions as within-subjects measures. Results indicated that frequency was significant (F(6.441, 978.975)=965.712, p=<.001>2 =.864). This result was expected because of the magnitude of the REUR changes across frequencies. Ear tested was not significant (p=.159, η2= .013), meaning results did not change whether we were testing the right or left ear.
For the purposes of this study, we were most interested in the significance of Placement Method. When the four sets of measures (ie, VA, VA-retest, PG, PG-retest) were compared, results indicated that placement method was not significant (p=.966, η2=.002) indicating that the measures within repetitions and between test methods did not differ. The average REUR difference at each frequency is presented in Figure 6 (PG-VA). Descriptively, these results show less than 1.6 dB difference between the visually assisted and Probe Guide measures out to 12,500 Hz. The 95% confidence interval shows that differences between the two placement methods were less than 2.5 dB up to 8,000 Hz, and less than 3 dB up to 12,500 Hz.
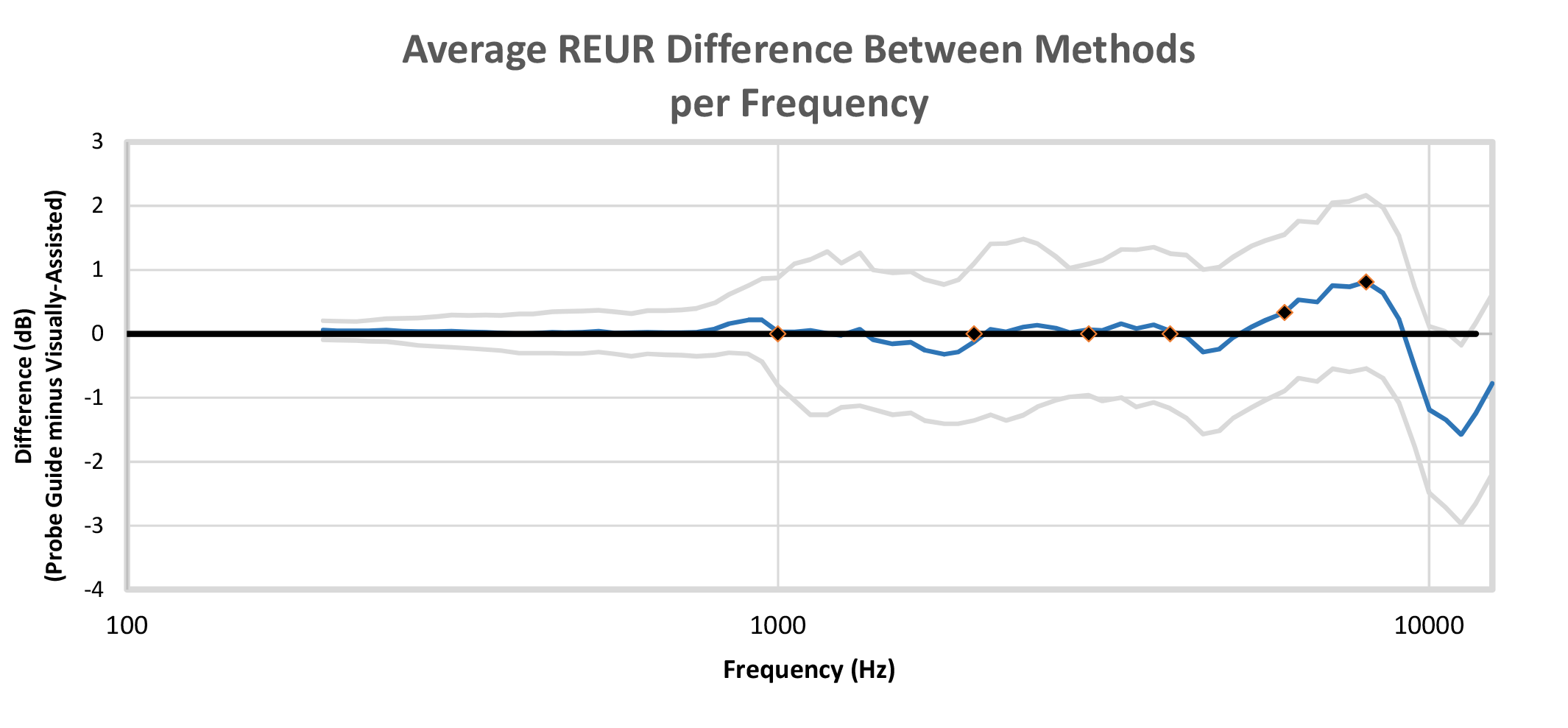
Figure 6. Average real-ear unaided response (REUR) differences across frequencies for a 65 dB SPL pink noise input signal with 95% confidence intervals (PG minus VA). Audiometric frequencies of 1,000-8,000 Hz marked for reference. Results show that, on average, differences were less than 1.5 dB out to 10,000 Hz. The 95% confidence intervals show differences remained below 2.5 dB up to 8,000 Hz and below 3 dB up to 12,500 Hz.
Probe tube insertion depth measurements. Probe tube insertion depths (Figure 7) relative to the intertragal notch for males ranged from 29-41 mm for both placement methods (mean = 33.9 mm using VA; mean = 33.7 mm using PG). For the female group, the probe tube depth ranged from 25.5-34.5 mm (mean = 30.2 mm) using the visually assisted and a range of 25-35 (mean = 30.0 mm) using Probe Guide. As expected, probe tube depth by gender was significantly different (F(1, 0.584)=5995.110, p<.001>2=.345). However, when the probe tube insertion depths for the 40 ears (20 left and 20 right) were compared across the four placement conditions (ie, VA, VA-retest, PG, PG-retest), the ANOVA results indicated Placement Method was not significant (F(2.447, 95.424)=.780, p=.485, η2 =.020), nor was Method by Gender (F(2.467, 93.727)-.669, p=.545., η2=0.017).
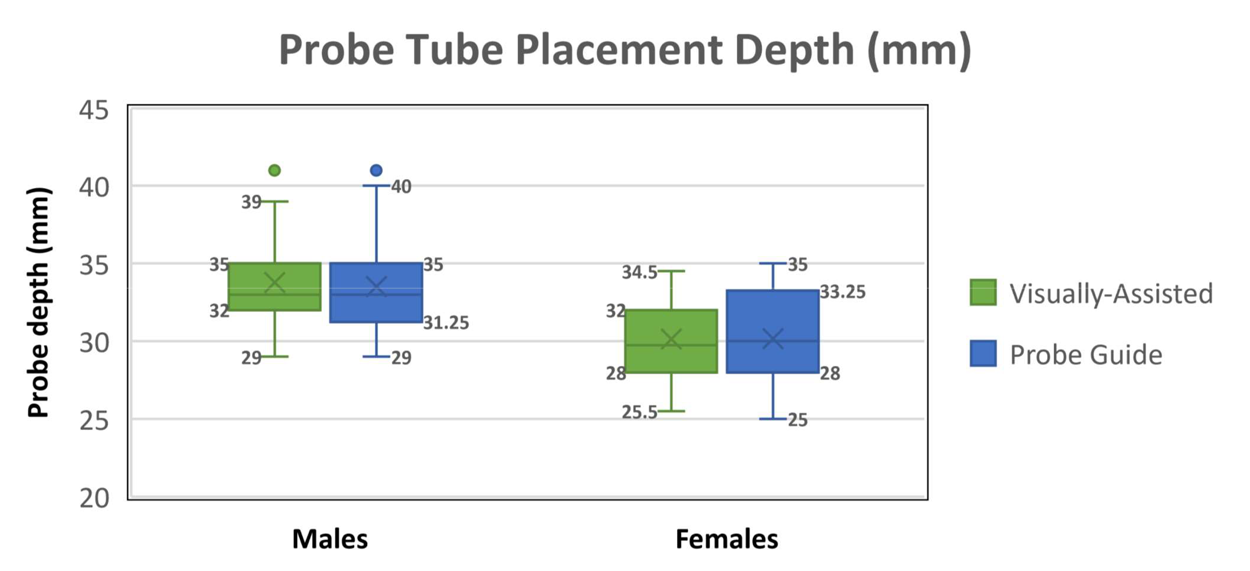
Figure 7. Probe tube insertion depth relative to the intertragal notch for 20 male and 20 female ears. Each box represents the probe tube depth mean (x) median (—); measurement range (I), first quartile (bottom of box), third quartile (top of box), and outliers (•).
Observational reporting of the probe tube placement methods. Of the 160 probe tube placements, there were no reported incidences of contact with the tympanic membrane or discomfort reported using either of the two placement methods. Following each use of Probe Guide, the experienced clinician viewed and commented on the resulting placement. Of the 80 software-assisted Probe Guide placements, one placement was deemed to be too far away from the tympanic membrane (3 mm farther than the visually assisted method) and 5 placements were deemed to be at an appropriate distance but likely too close to the tympanic membrane when inserting a hearing aid or foam tip (2-3 mm closer than the visually assisted method).
